Introduction
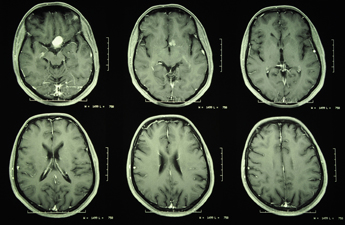
Meningiomas are benign tumours that arise from the linings of the brain (the meninges). There are no specific predisposing factors to these sorts of tumours. They can occur anywhere along the inner surface of the meninges, either within the brain cavity or within the spinal canal. The fact that they are benign means that they grow very slowly and as a result, patients will often have had these for many years before they are diagnosed with the tumour.
How do they present?
The symptoms that they present with are a function of both their size and site. If a meningioma is growing in a part of the brain cavity adjacent to a relatively ineloquent (non-functional) part of the brain, it can become quite large without causing symptoms.
In other more sensitive areas of the brain, meningiomas can create symptoms very early, either due to pressure on the brain or irritation of nerves exiting from the brain. As a consequence of this, there is no “typical” symptom arising from meningiomas. Due to their varied size and site, there is no single treatment solution. The neurosurgeons of the Brain and Spine Clinic would consider all of these factors including your medical history to formulate a very individualised treatment for your meningioma.
What are the management options?
Very often, if you have a small meningioma with minimal or no symptoms (meningiomas are not infrequently diagnosed as incidental findings when undergoing a brain scan for other reasons), the most sensible first management option is to simply re-scan you to see whether indeed yours is a tumour that is actively growing or not.It is certainly true that not all meningiomas grow and can remain static in the long term. Even with growing meningiomas, a growth rate of only 1 or 2 mm a year is typical, and therefore the initial interval before your first follow up scan is usually 6 months. This interval can be increased if the tumour remains stable on follow up scans and if this continues, no further active treatment may be necessary.
The management of your tumour will not only be discussed between you and your surgeon, but also at an appropriate Multidisciplinary Team (MDT) Meeting . These are held at Salford Royal Hospital, with a team of experts with a huge combined experience of managing such problems. Your surgeon will convey the outcome and recommendations of this meeting to you. Whilst this will provide you with all the information you require about your meningioma, as well as a detailed analysis of the advantages and disadvantages of all management options, the most important factor in the final decision is you. Your personal opinion of what is best for you is undoubtedly the most relevant aspect of how you will be managed.
Treatment - Surgery or Radiotherapy?
The bedrock of meningioma treatment, in those cases where treatment is required, is surgery. It is emphasized that as described above, it may be that if your meningioma falls within the appropriate category, it may be possible to simply observe it over a period of time to see if it progresses. In terms of treatment, the options are radiotherapy and surgery. It would be fair to say that for the majority of intracranial and spinal meningiomas, the default position for treatment is surgical resection. This is aimed to physically remove the tumour, decompressing the adjacent brain and in the majority of cases providing cure.
In terms of surgery, the surgical approach is designed to maximise the surgeon’s access to the tumour whilst minimising retraction of the adjacent brain. This approach is highly individualised to the tumour and would be discussed with you by the neurosurgeon you see at the Brain and Spine Clinic. The approach is designed to allow the surgeon to physically remove the tumour in as safe a fashion as possible and, therefore, with minimal risk of harm to the surrounding brain, nerves and blood vessels.
In certain cases, radiotherapy may be an option. These would typically involve meningiomas in areas of the brain where surgical resection is either impossible or exposes the patient to excess risk. The second situation in which radiotherapy may be required is that in which the tumour is of an unusually aggressive nature. The vast majority of meningiomas are benign (World Health Organisation [WHO] Grade I) but occasionally the meningioma is WHO Grade II and even more rarely WHO Grade III (malignant meningioma). Should the meningioma not be Grade I, it may be advised that adjuvant radiotherapy should be given to minimise the chance of recurrence.